

INTRODUCTION
Old age ought to be considered a normal, inevitable biological phenomenon.
Oral health is gaining global attention as a result of it's closely coupled to general health and the quality of life.
As a result of the advances made in medication and public health measures within the second half of the 20th century, there's a considerable increase in the lifetime of man.
As the world population ages, attention services for senior people have been further developed to boost their health and quality of life.
Thus, coming up with treatment for the senior dental patient includes an understanding of the chronic malady's the patient lives with daily, as this plays a vital role within the acceptance and success of the dental treatment plans.
The World Health Organization outlined health as a dimensional construct: “a state of complete physical, psychological, and social well-being and not simply the absence of disease or infirmity”.
GERONTOLOGY
The study of the physical and psychological changes that are incident to maturity is termed gerontology and care of the aged is called clinical gerontology or geriatrics.
Geriatric dental medicine or Gerodontics also can be defined because the delivery of care to older adults involves the diagnosis, bar associated treatment of issues related to traditional ageing and age-related diseases as a part of a knowledge base team with different health care professionals.

CLASSIFICATION OF ELDER PATIENTS
| AGE (years) | CLASSIFICATION |
|---|---|
| 65 to 74 | New or Young elderly |
| 75 to 84 | Old or Mid old |
| Above 85 | Older or Oldest old |
ORAL HEALTH
oral health is associated with Health-Related Quality of Life major efforts are created to develop instruments for the measuring of Oral Health-Related Quality of Life (OHRQoL) affects one’s general well-being which oral health is an integral part of general health, it may be thoroughbred that oral health is, in part, to blame for the overall state of well-being.
This is often particularly necessary within the elderly.
CHALLENGES IN OLDER PEOPLES
The management of older patients needs not solely an understanding of the medical and dental aspects of ageing
However additionally several different factors similar to
- Ambulation
- Independent living
- Socialisation
- Sensory function.
Several barriers could interfere with
- Providing previous patients with care
- Heightened dental complexity
- Multiple medical conditions
- Diminished useful standing
- Loss of independence
- Unenlightened attitudes regarding dental care in old age
- Restricted finances.
These issues may be overcome in the dental profession by education, clinical programmes, analysis agendas, and legislative advocacy.
RELATION BETWEEN ORAL HEALTH IN SYSTEMIC DISEASES
Diseases seen in senior patients are
- Cardiovascular diseases
- Diabetes
- Respiratory diseases
- Blood dyscrasias
- Different general diseases
- Dementia
- Pneumonic infections
- Some varieties of cancer
- Excretory organ disease which has relation with dental manifestations..
WIDELY PROPOSED MECHANISM
| Mechanisms | Mechanisms explanation |
|---|---|
| Inflammatory mechanisms | Inflammation derived from the host response against periodontal pathogens originates molecules that gain access to the circulatory system, manufacturing general inflammation with tube and different repercussions |
| Bacterial mechanisms | Microorganism or bacterial product directly invade the tissues of the organism |
| Vascular mechanisms | Presence of periodontal pathogens within the circulation , inflicting blood platelet aggregation and atheroma/small clot formation |
Cardiovascular diseases and uncontrolled diabetes could exacerbate periodontal inflammation.
Periodontitis is probably going to develop as a result of a depressed system and is planned because of the sixth complication of diabetes.
Older people are additional at risk of oral diseases because of increase in chronic conditions like diabetes, heart diseases, respiratory problems, nutritional deficiencies and physical & mental disabilities
Considering this disease's senior population forms a definite cluster in terms of provision for dental care.
Infective endocarditis, another common disease found in elderly patients, has association with periodontitis.
The bacteria like viridans streptococci ordinarily found in oral cavity, whereas the microorganism found in plaque like
- Actinobacillus actinomycetemcomitans
- Eikenella Corrodens
- Fusobacterium Nucleatum
- Bacteroides Forsythus
are isolated from the blood sample of Infective carditis patients.
The role of native/systemic inflammation of periodontal origin within the pathologic process of Alzheimer’s disease (AD) isn't absolutely understood, however there's substantial scientific proof of its potential implication in the vascular damage.
The general presence of inflammation factors derived from local inflammation in moderate–severe periodontitis (eg, interleukin-1β, interleukin-6, tumour necrosis factor-α, and C-reactive protein, etc) has been involved in brain inflammation and future neurodegeneration in AD patients.
Respiratory infections are sometimes caused by oropharyngeal and periodontal microorganism and bacteria.
The most reason behind respiratory infections and microorganism respiratory disorder in adults is aspiration of oropharyngeal bacteria.
This small flora inhabits inadequate oral hygiene leading to formation of plaque further surviving as a reservoir for respiratory pathogens.
The other common disease rheumatoid arthritis (RA) is seen in aged patients.
This RA has a similar characteristic of disease as there's destruction of arduous and soft tissues as a results of inflammatory response.
However, the interrelatedness furthermore as association between RA and periodontitis has not been proved.
Type one and Type two DM have distinguished dental manifestations reminiscent of loss of periodontal attachment, gingival and periodontal symptoms and early loss of teeth.

HEALTH ISSUES IN OLDER PATIENTS
Among adults sixty five years previous or older, missing natural teeth associated
- Chronic oral diseases
- Dental caries
- Periodontal diseases
- Oral infections
- Oral tissue layer lesions
- Temporomandibular disorder
- Oral cancer
Diagnosis and treatment coming up with for the senior should embrace concerns of the biological, psychological, social and economic status of the patient additionally to the apparent dental issues
DETAILY ABOUT ORAL ISSUES IN OLDER PATIENTS
TEETH COMPONENTS CHANGES PRECEDING WITH INCREASING AGE
| Tooth part | Changes in preceding with age |
|---|---|
| Enamel | The perikymata and overlapping lines are lost, giving the enamel surface a flat look with less detail than in recently erupted teeth. Wear and attrition have an effect on the tooth form.The altered surface structure offers the teeth in older people a distinct pattern of light reflection, that causes a modification within the determined color. enamel don't exhibit any physiological turnover of their components. |
| Dentin | Changes in the dentin, each in amount (thickness) and quality additionally lead to a gradual loss of transparency. Changes such as Continued growth, observed as physiological secondary dentin formation and Gradual obturation of the dentinal tubules referred to as dentin sclerosis. |
| Cementum | Cementum apparently continues to be set throughout life, however the speed of formation diminishes with age. underneath some circumstances, excess amounts of cementum is also formed (hypercementosis) related to accelerated elongation of an unopposed tooth or to an inflammatory stimulus. |
| Pulp | The blood supply, as well as the wealthy plexus of capillary loops within the subodontogenic region, is greatly reduced. These changes are vital as a result of the pulp can not be expected to own an equivalent reparative capability because the younger teeth. microscopy of previous pulps has shown loss and degeneration of each myelinated and unmyelinated nerves and so affected the healing capacity of pulp. Pulp calcifications also are found to extend in frequency, variety and size with age. Diffuse calcification and narrowing of the foundation canals with increasing age. |
DRY MOUTH
The larger life expectancy of populations has additionally accumulated the importance of xerostomia as a health issue.
A high prevalence of xerostomia associated exocrine gland hypofunction has been found in vulnerable older people.
The diminished operat of the salivary gland is often related to aging. The implications of disordered salivary gland maintenance of oral health.
The presence of saliva protects the oral fissure of the upper airway and alimentary canal and facilitates various sensorimotor phenomena.
With advancing age, there's an atrophy of acinar tissue, a proliferation of ductal parts and a few chronic changes within the major salivary glands.
These alterations tend to occur linearly with increasing age. Minor exocrine glands additionally endure similar chronic changes with advancing age.
Thus, there's a normal, uniform decrease within the acinar content of secretion gland tissue incidental to the aging process.
The absence of saliva has several harmful consequences to the host.
Etiologic factors embody polymedication (especially with antihypertensives, antidepressants, and antipsychotics), poor general health, female sex, and older age.
There are various studies on the impact of dry mouth syndrome on the oral and general quality of life of the older as a result of it's one in all the issues most often reported, and treatment success rates are low.
It seems that decreased secretion flow doesn't uniformly accompany the aging in healthy persons.
These useful observations contrast with morphologic changes seen in aging salivary glands.
One rationalization that has been hypothesized to account for this is often that salivary glands possess a functional reserve capacity, sanctionative the glands to keep up a continuing fluid output throughout the human adult life span.
Various approaches are studied, together with products specifically indicated for dry mouth, appreciate artificial saliva and saliva-stimulating medicine (pilocarpine), however the outcomes haven't been encouraging.
Palliative measure include
- Rectification of the underlying reason behind xerostomia (drugs, diabetes, etc)
- The rejection of dry hot environments
- Dry foods
- Drugs
- Alcohol
- Smoking
- Among alternative situations/activities that will increase dryness
- Regular dampening of the mouth with
- tiny sips of water
- lip balm
- olive oil ect.,
Individuals with dry mouth need preventive measures against the results of the absence of saliva, together with caries, periodontal disease, and candidiasis.
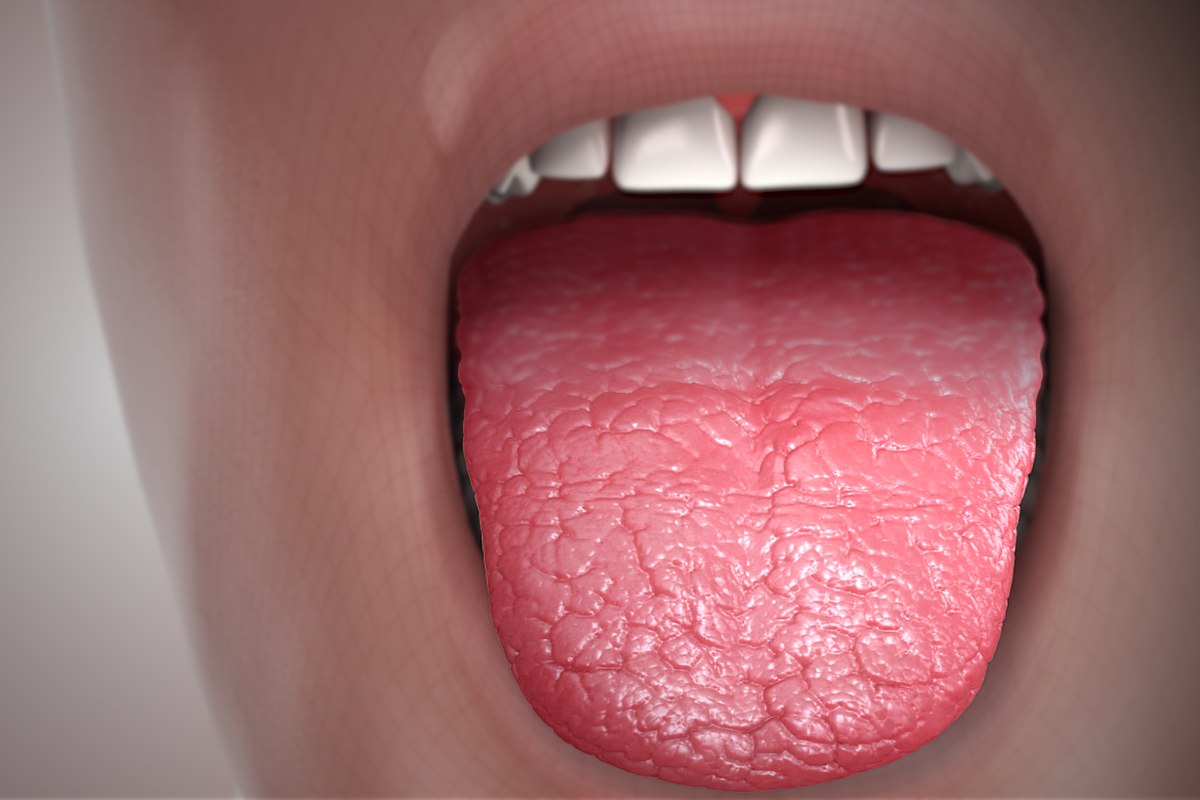
Dry mouth
Photo credit: scientificanimations.com (wikipedia commons)
PERIODONTAL DISEASE
Periodontal disease within the aged doesn't seem to be a specific disease however the results of a chronic adult periodontitis since adulthood though age-related changes are documented in the periodontium of elders, these changes don't appear to be the reason for periodontitis in the elderly.
Increased severity of periodontal diseases with age has been concerning the length of your time the periodontal tissues have been exposed to the dentogingival plaque and is considered to mirror the individual’s accumulative oral history.
However, the condition of the periodontium to plaque-induced periodontal breakdown is also influenced by the aging method or by a selected health problems of the aging patient.
The bigger quantity of plaque recovered within the elderly subjects can be due, in part, to a bigger space for plaque retention as a result of the gingival recession.
Epidemiological knowledge on periodontal disease (a chronic infectious disease that affects tooth support tissues, as well as gingiva and alveolar bone) has shown that the foremost frequent findings among the elderly are the buildup of bacterial plaque with consequent periodontal disease and delicate or moderate alveolar bone loss.

Plaque was attached to the tooth structure
Photo credit: Francisco B. Teixeira, Miki T. Saito, Filipe C. Matheus, Rui D. Prediger, Elizabeth S. Yamada, Cristiane S. F. Maia, Rafael R. Lima1 (wikipedia commons)
ORAL CANCER
Oral cancer represents a serious threat to the health of adults and also the aged in each high- and low-income country.
It includes lip, oral cavity, and pharyngeal cancer, and is the eighth commonest cancer worldwide. Incidence and mortality rates are higher in men than in women.
The prevalence will increase with older age, and oral cancer is of specific concern among over-65-year-olds.
Variations among countries are due to variations in risk profiles and to the supply of and accessibility to health services, among others.
Oral cancer is often treated with surgery, radiotherapy, and/or chemotherapy, and advances have led to a reduction in mortality and to an exaggerated variety of survivors.
The cancer and its treatment can each be to blame for major anatomical changes within the oral cavity and also the alteration of basic functions, as well as speaking, chewing, and/or swallowing, considerably impairing the standard of lifetime of survivors.
A multidisciplinary approach is crucial for reducing the impact on patients, with a vital role for dentists. dental care before, during, and when treatment can facilitate to keep up or improve the quality of life of carcinoma patients.
However, the short fundamental measure between identification and treatment, and the lack of coaching during this field by dental professionals, are among the barriers to be overcome within the implementation of this proactive approach.
Despite the said poor oral health conditions of the elderly, this can be often not matched by their self-perception of oral health.
Hence, it's very important to go on the far side of clinical aspects in coming up with the dental treatment of this age group.
DENTAL CARIES
Caries remains a serious oral pathological state among the older for numerous reasons
The rise in treatment and maintenance of teeth instead of their extraction
Age-related secretion changes; a poor diet
Exposure of the basis surface by gingival recession
A bigger chance of drug treatment with dry mouth as a facet effect.
In general, there's high prevalence of tooth loss thanks to caries, reflective the actual fact that the treatment offered to this point has mostly been extraction of the affected tooth.
This routine restoration procedure is to get rid of the least potential amount of decayed tooth and to concentrate on remineralizing the affected tooth with fluoride, with the aim of rising the standard of lifetime of patients by maintaining their natural teeth and avoiding the necessity for removable or fixed prostheses.
MOBILE DENTISTRY ONE OF THE EFFECTIVE TOOL IN GERIATRIC DENTISTRY
Portable dental equipment includes comparatively light-weight and simply movable dental chairs, x-ray units, and moveable dental drills.
Mobile dental units are motorized vehicles that are self-contained dental operatories with dental chairs, x-rays units, and stuck dental drills.
Geriatric patients were additionally hospitalized when their dental-related ER visit and more likely to finish up in an exceedingly long-/short-term care facility (rather than come home), that incurs monumental sequent charge.
In geriatric patients, Portable dental dentistry could conjointly reach the positioning of an oversized leader to supply services to the workers (of all ages) with bottom disturbance to their work day.
Some 1.4 million emergency room visits every year are concerning basic dental issues like dental caries and tooth abscesses, and 175,000 hospitalization days each year are related to a primary diagnosis of a basic dental condition.
Portable dental dentistry provides several edges to patients and suppliers and has been extremely effective in elderly.
Opportunities exist to deliver care through mobile clinics or moveable dentistry at the placement of an oversized employer.
If a dental team will overcome the barriers of entry into this field, a highly satisfying and economical work environment is established, with sturdy benefits of convenience to the patients they serve.
PREVENTIVE MEASURES

IMPORTANCE OF BRUSHING AND TYPE OF TOOTHBRUSH IN ELDERLY PATIENTS
The elderly person ought to be helped to develop the ability to brush effectively and thoroughly.
Those that have diminished manual dexterity could like the employment of
- Traditional mechanical toothbrushes
- Rotary electric toothbrushes
- Manual brushes that are custom-made or customized for every person.
Many elderly persons are hampered in their efforts of effectively performing plaque management procedures by physical disabilities that end in the shortage of manual dexterity or impaired vary of motion of the wrist, elbow or shoulder.
Their plaque removal efforts are also increased by use of an electrical device or by adaptation of manual plaque control aids.
If an older person’s grip is weakened by a condition that appreciates arthritis, they encounter problems grasping the slender handle of a traditional toothbrush, floss holder, or different home care aid.
To modify the patient to perform effective plaque removal, the handles are often enlarged or designed up so it can be grasped simply and comfortably.
Persons with gingival recession should be taught to look at bound precautions to avoid more recession or cemental abrasion.
These could embrace the employment of an additional soft toothbrush, use of light pressure, modification of the brushing method.
The plaque retention within the elderly is exacerbated by the presence of restorations, missing teeth and gingival recession.
Electric toothbrush
This is often a useful aid for the aged once used properly.
These devices have enlarged handles, which can be grasped a lot more simply than the quality manual toothbrush handle.
The foremost advantage is that they're motor driven, so requiring very little or no arm or carpus movement, and also have to be compelled to create consistent movements.
A number of the electrical plaque removal devices are designed in such the simplest way that the action stops if an excessive amount of pressure is applied.
However, an elderly one who has congenital cardiovascular disease or any condition affecting heart valves ought to be cautioned concerning the danger of developing acute microorganism carditis secondary to soft tissue trauma caused by improper use of electrical devices.

CARE OF DENTURE THOSE WHO ARE WEARING DENTURES
The wearing of removable dentures may additionally negatively influence plaque accumulation.
In addition, they usually face problems in mechanical removal of plaque due to reduced adroitness or impaired vision or due to physical limitations related to conditions like stroke, Parkinson’s illness or severe arthritis.
Elderly persons who wear full or partial dentures should be educated to wash these appliances in an exceedingly method that's effective.
Immersion of denture in cleansers is the suggested method that ensures safety against injury of the denture material.
The patient ought to be instructed perpetually to brush and rinse the denture completely before and once soaking in immersion cleans.
The elderly who wear dentures ought to be educated to correct home care of each denture and tissues so that they rest similarly because they would like for continued skilled care.
The tissues are often prevented from harm by avoiding sporting the denture constantly. an instruction for the removal of the denture whereas retiring for the night is essential.
The cleanup and massaging of the tissues beneath a denture a minimum of once daily will increase circulation and therefore enhances the health of those tissues.

EFFECTIVE MOUTHWASH FOR ELDERLY PEOPLE
Fluoride mouthwash
1. It inhibits the development of caries by being incorporated into the developing enamel within the kind of fluorapatite.
2. It enhances remineralization of the unhealthy enamel.
3. Halide has an anti-bacterial action.
Chlorohexidine mouthwash
1. It's primarily indicated for gingivitis.
2. It is effective against a spread of plaque bacteria, so enhancing the patient’s mechanical plaque management efforts for patients with physical and mental disabilities.
3.It conjointly reduces oral mucositis and monilia disease in immune suppressed patients appreciate those on intensive chemotherapy
NUTRITIONAL REQUIREMENTS FOR OLDER PATIENTS
Good health is achieved by assimilation of a healthy diet and this more helps in maintaining health of oral exhausting (teeth) and soft tissues.
The most well-liked technique of brushing for many elders is sulcular brushing with soft toothbrush (Bass method).
The physical, physiological, psychosocial, and emotional characteristics of the senior establish them as a population cluster at high risk of poor nutrition.
Their diets are oft monotonous, with a often energy and nutrient content and deficiencies in
- Calcium
- Zinc
- Magnesium
- Iron
- Vitamin D
- Vitamin B6
- Vitamin B12
- Vitamin E
- Thiamin
- Retinol
- Carotenes
- Folic acid.
Deficient chewing is said to cause tooth loss, a lack of saliva, mastication force, and disorder issues.
Some native studies have indicated that people with mastication problems avoid contemporary fruits and vegetables, “well-done” meat, and even bread,preferring soft, simply cuttable food that may usually raise sugar and fat consumption to levels on top of recommendations, increasing their risk of cardiovascular diseases and metabolic syndrome.
Many toothless elderly believe mistakenly that after all their teeth are extracted they do not have to be compelled to be anxious regarding oral health.
Some of the physical factors influencing biological process includes
- Sensory alterations
- Reduced thirst
- General deterioration of physiological functions
- Body composition changes
- Chronic diseases (including depressive states, powerfully associated with malnutrition)
- Polymedication
- Constipation
- Disability
- Reduced physical activity.
CONCLUSION
Effective oral care to regulate plaque and promote oral tending includes correct tooth brushing and cleanup and annual dental check-ups.
Medical care to market oral health is crucial to help the institutionalized senior population meet an appropriate level of oral health and increase their awareness of oral healthcare.
To enhance the motivation to frequently visit the dentist, an educational program ought to be developed for each institutionalized resident and caregivers.
An educational program should aim to extend the notice of oral care and hygiene to improve oral care practices.
REFERENCE
- Razak, P. A., Richard, K. M., Thankachan, R. P., Hafiz, K. A., Kumar, K. N., & Sameer, K. M. (2014). Geriatric oral health: a review article. Journal of international oral health : JIOH, 6(6), 110–116.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4295446/
- Gil-Montoya, J. A., de Mello, A. L., Barrios, R., Gonzalez-Moles, M. A., & Bravo, M. (2015). Oral health in the elderly patient and its impact on general well-being: a nonsystematic review. Clinical interventions in aging, 10, 461–467. https://doi.org/10.2147/CIA.S54630https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4334280/
- Gupta, S.; Hakim, M.; Patel, D.; Stow, L.C.; Shin, K.; Timothé, P.; Nalliah, R.P. Reaching Vulnerable Populations through Portable and Mobile Dentistry—Current and Future Opportunities. Dent. J. 2019, 7, 75.
- Pradhan, Manjusha & Sonarkar, Snehal & Shenoi, Pratima & Uttarwar, Varsha & Mokhade, Vidya. (2016). Geriatric Dentistry-an Overview. International Journal of Oral Health Dentistry. 2. 26-28. 10.5958/2395-499X.2016.00004.6. https://www.researchgate.net/publication/299536361_Geriatric_Dentistry-an_Overview
- Wong, F., Ng, Y., & Leung, W. K. (2019). Oral Health and Its Associated Factors Among Older Institutionalized Residents-A Systematic Review. International journal of environmental research and public health, 16(21), 4132. https://doi.org/10.3390/ijerph16214132
Photo credits









0 Comments