

INTRODUCTION
From time to time, numerous different strategies of tissue destruction had been employed, chemicals, irradiation via means of X-rays and high-frequency electric current being some of them.
Ideally, any approach in opposition with the surgeon's scalpel has to be painless, produce minimum harm to the surrounding tissues, be selective against, for example, malignant cells, be localized and readily controllable and promote fast and uneventful healing.
Cryosurgery has made a solution to all of this.
Cryosurgery is likewise used to deal with tumors inside the body.
For inner tumors, liquid nitrogen or argon gas is circulated through a hole device referred to as a cryoprobe, this is positioned related to the tumor.
Liquid nitrogen has become the most sizable refrigerant due to its extensive availability, loss of explosive capacity compared to liquid oxygen, ability to freeze up to -197 °C and inevitable effect.
Cryogen has observed applications in treatment of nephron-sparing kidney cancers, bone tumors, hepatocellular carcinomas and prostate cancer.

CRYOTHERAPY AND IT’S MECHANISM
Cryosurgery (also called cryotherapy) is the use of extreme cold produced by liquid nitrogen (or argon gas) to destroy abnormal tissue.
Cryosurgery is a method of local destruction of tissues by freezing in situ "Cryosurgery" is derived from the Greek word "Kryos," that is, frost, thus literally meaning frost surgery.
The local application of low temperature was probably first used as a means of analgesia by the ancient Egyptians.
Cryosurgery is not simply the application of freezing temperatures to tissue. The aim of cryosurgery is to kill and destroy cells.
Cryotherapy is a thermal ablative modality that utilizes cycles of rapid cooling and thawing to induce tissue destruction with a refrigerant, usually a liquefied gas like nitrogen or nitrous oxide.
Cryotherapy employs a non-contact method, wherever a cryogen is sprayed on the targeted mucous membrane leading to mortification of superficial esophageal mucosal layers.
Since cryotherapy is targeted, the targeted space gets deeper ablation compared to alternative techniques.
There are numerous styles of cryogens available, as well as
- Nitrogen gas
- CO2 acid gas
- Other compressed gases
however the foremost common cryogen far and away is liquid nitrogen.
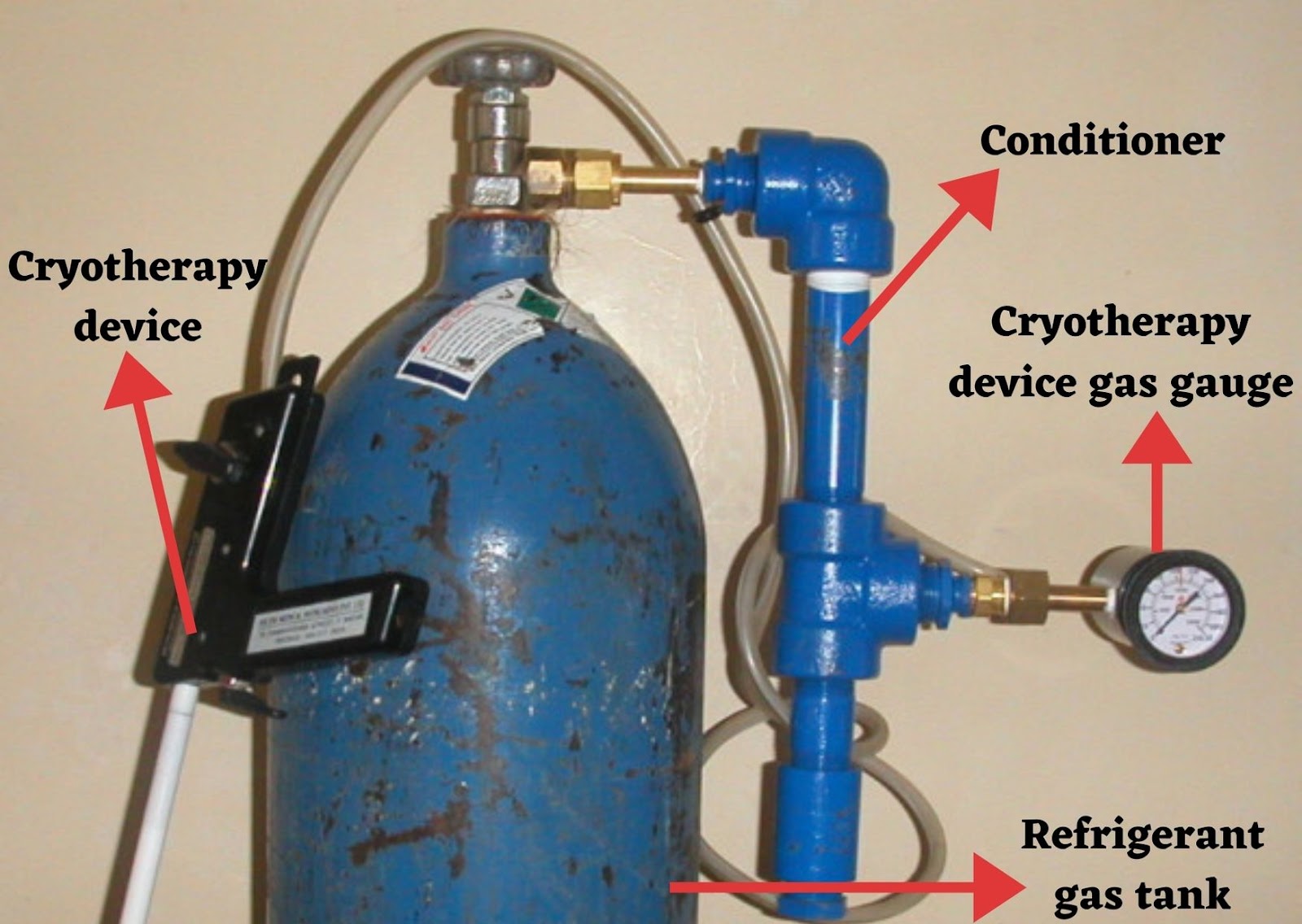
Photo credit: Seamans, Yancy & Sellors, John & Broekhuizen, Fredrik & Howard, Michelle. (2006). Preliminary report of a gas conditioner to improve operational reliability of cryotherapy in developing countries. BMC women's health. 6. 2. 10.1186/1472-6874-6-2.

Cryogun ( Handy apparatus which does not need cylinder and other heavy apparatus)
Photo credit: Warfieldian (Wikimedia Commons)
MECHANISM
| Direct effect | Indirect effect |
|---|---|
| Cellular enzyme system operates optimally over a slender temperature range, sudden cooling acts as an inhibitor. This renders the cells more liable to the metabolic disturbances. | Ischemic gangrene created by vascular stasis and microthrombus formation may be a vital a part of the cryodestructive process. Large vessels still function, though with enlarged permeability. |
| The additional rapid the cooling rate, the larger the ice crystals formed, associated incidentally the greater the degree of adhesion of the tissues to the probe. large ice crystals turn out physical disruption of cell membranes. | Massive release of pathological cell antigens and/or changes to the substance nature of the frozen and thawed cells, so creating them at risk of host surveillance mechanisms. |
| During the cooling method, the membrane becomes extremely permeable and permits mass transfers of ions, leading to damaging changes within the ionic composition of the cell. | |
| These temperature changes have an effect on many intra- and extracellular mechanisms resulting in semipermeable membrane disruption and thrombi formation within the blood vessels causing programmed cell death and ischemia. | |
| Crystals dissolve due to raised temperatures, making a reverse osmotic gradient. Water re-enters the cells, inflicting swelling and rupture. | |
| When the cooling process stops and therefore the tissues are allowed to rewarm, more damaging effects might take place. |
USE OF CRYOGENS IN ORAL DISEASE
It may be used as single treatment for
- Mucocele
- Trigeminal neuralgia
- Leukoplakia
- Hemangioma
- Pyogenic granuloma
- Human Papillomavirus lesions
- Actinic cheilitis
- Lichen planus
- Fibromas
It may be used as complementary treatment for bone lesions with high recurrence rates, like
- Ameloblastomas
- Myxomas
- odontogenic keratocyst
- Ossifying fibroma
- Central large cell lesions.
Based on information reported within the literature and regular practice, surgical procedure may be a safe and extremely effective procedure in the treatment of lesions occurring in the oral and maxillofacial region.
CRYOSURGERY IN ORAL LESION
Oral mucosal lesions are usually classified into surface lesions typically involving the epithelial tissue and superficial connective tissue of mucosa.
These lesions include
- white, pigmented, and vesicular-ulcerated erythroderma lesions
- Reactive soft-tissue enlargements which can increase and reduce (fluctuate) in size and typically eventually regress
- Soft-tissue tumors that are characterised by being persistent and progressive which don't resolve without treatment.
Cryosurgery include
- Relative lack of discomfort and pain (decreases nerve conductivity speed)
- Absence of bleeding (vasoconstriction)
- Negligible to no scarring
- Easy application
- Preservation of inorganic structures of bone
- Terribly low incidence of infection (decreases the metabolic rate, thereby drop-off secondary injuries because of lack of oxygen), and being a lot localized in action.
It will be repeated with non permanent side effects.
Cryogenic apparatus has been accustomed to treat minor oral lesions with satisfactory results because it provides higher control with fast freezing of the desired region.
Moreover, it's convenient to use as it is lightweight, moveable and may be controlled with an on-off switch.
Hence, cryotherapy is terribly helpful for oral lesions because the oral tissue layer is wet and smooth, that makes it a perfect site for freezing.
CRYOTHERAPY IN ORAL MUCOSITIS
Oral mucositis (OM) refers to erythroderma and painful lesion lesions of the oral tissue layer discovered in patients with cancer, who are treated with chemotherapy, and/or with radiation therapy.
OM is a painful complication that causes dysphagia, alterations in taste, weight loss, and secondary infections.
These complications can considerably complicate treatment, extend hospitalization, and decrease the patient’s quality of life (QoL).
The National Cancer Institute (NCI) published Common terminology Criteria for Adverse Events (CTCAE). It includes separate subjective and objective scales for mucositis:
- Grade 1—Erythema of the mucosa
- Grade 2—Patchy ulcerations or pseudomembranes
- Grade 3—Confluent ulcerations or pseudomembranes; injury with minor trauma
- Grade 4—Tissue necrosis; vital spontaneous bleeding; serious consequences
- Grade 5—Death.
It's necessary to stay in mind, however, that once therapy or/and radiation are applied, oral membrane lesions also are attainable in different erosive diseases, corresponding to oral candidiasis, herpes simplex virus infection, acute Graft-versus-Host disease.
Cryotherapy was performed by holding a piece of ice within the mouth throughout the therapy infusion.
Cold prevents blood flow to the oral cavity, leading to reduced cytotoxic chemotherapy access to the mucosal tissues, that reduces the chance of OM, however additionally reduces the effectiveness of primary disease treatment.
Therefore, cryotherapy reduces the development and period of OM.
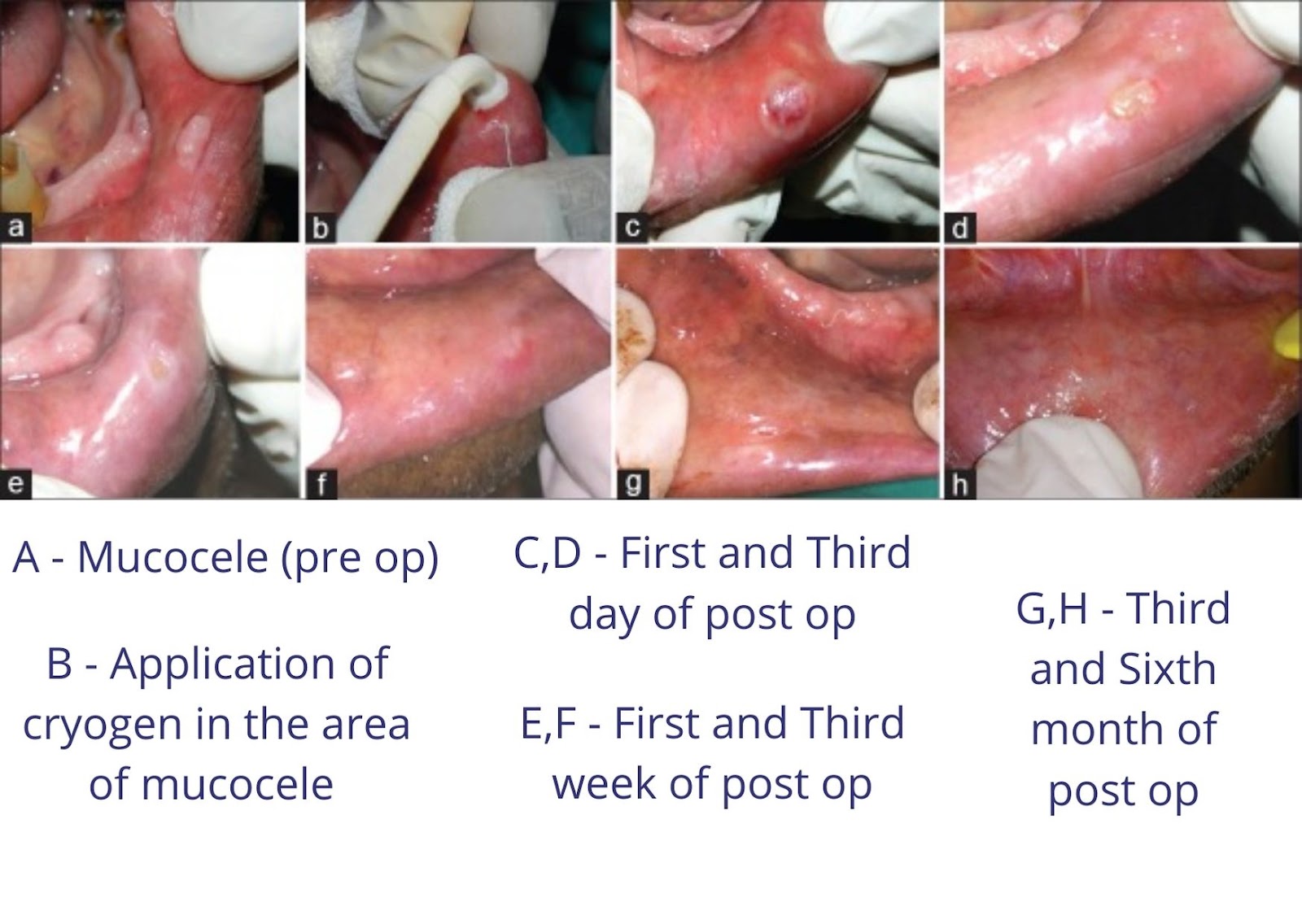
Photo credit: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6006886/bin/CCD-9-17-g006.jpg
LIMITATION OF ORAL CRYOTHERAPY
Cryosurgery of the tongue will produce swellings which may severely interfere with swallowing and sometimes respiration.Extensive surgery as within the case of widespread keratoses, severe pain are often troublesome and narcotic analgesics could also be required.
Healing of cryosurgery wounds happens slowly. However, they must be closely determined to beat the possibility of slow healing being regarding the persistence of a lesion, significantly if neoplastic.
Cryolesion can result in involvement of an inadequate quantity of tissue, leading to persistence of the pathologically modified epithelium and re-establishment of the lesion. So, one ought to be quite sure that ordinary tissues beyond the margins of the lesion are adequately frozen
CRYOSURGERY IN CANCER
Cryosurgery is at the best a way of localized tissue destruction in superficial accessible lesions.
Cryosurgery is additionally used to treat some sorts of inferior cancerous and noncancerous tumors of the bone.
Cryoablation ends up in direct cell death by removing heat.
Heat is transferred out of the growth and encompassing tissues making an
- Inner zone of direct cell death via lethal hypothermia whereas inflicting indirect cell death within the outer zone via apoptotic signaling.
- Outer zone, wherever cells aren't exposed to deadly below zero temperatures, injury to mitochondria results in delayed apoptotic cell-death.
The ratio of apoptosis to gangrene following cryotherapy considerably influences the immunostimulating effect.
Cryoablation induces a far bigger post-intervention response compared to radiotherapy because of this ratio which might be discovered by significantly increased levels of IL-1, IL-6, NFκB, and TNF-α post cryoablation.
Freezing instead preserves cellular ultrastructure and will increase plasma membrane permeability.
Cryoablation yields the discharge of intracellular debris, inflicting a unleash of cytokines that are related to the systemic inflammatory response syndrome that is yet another indication of the robust immune response induced by freezing primary cancer lesions .
Cryosurgery-induced tumour and cell death process includes 2 separate zones of destruction.
The inner zone of surgery ablation ends up in tumor coagulation necrosis and is understood as the central zone wherever cold temperatures reach −50°C.
The antigens of this central space are characterised by cellular breakdown and release of intracellular contents, however could so be cell surface antigens further as nuclear antigens.
The central zone cytokine milieu ensuing from cryosurgery is often a TH1 cytokine profile of
- IL-2
- IFN-γ
- TNF-α and
- IL-12.
These central zone antigens ought to then be processed via the Major histocompatibility complex class I resulting in a cytotoxic T-cell response.
The outer periphery zone of cryosurgery ablation ends up in cell death via apoptosis through extracellular freezing of fluid and osmosis, making a shift of fluid from the intracellular to the extracellular microenvironment that pushes the immune response to the unfavorable TH2 cellular response.
It should cut back the chance of joint harm in comparison with additional in depth surgery, and facilitate reducing the requirement for amputation.
Rapid freeze and thaw cycles cause immediate effects of deceleration cellular metabolism and phase transition intracellular water.
Subsequently, ice formation ends up in disruption of cellular membranes and organelle dysfunction and eventually cellular apoptosis.
There is extremely restricted information on the utilization of cryotherapy for the treatment of squamous cell cancer (SCC) or squamous dysplasia.
Its use has been chiefly confined to continual or persistent growths following surgery and/or radiation.
Consistent with Holden, cryosurgery is the treatment of selection in recurrent nasopharyngeal carcinoma.
In cryotherapy, the tissue design of the superficial squamous layers is left comparatively intact, and there's less tissue damage, which can underlie the reduced stricture formation rate with this modality.
Surgical excision and radiotherapy are well tried and carry a good prognosis, in sure circumstances, there is danger to encompassing structures, for example, Basal cell ulcers at the inner canthus.
Similarly, in cases wherever there are multiple lesions, cryosurgery could be a sound various to surgery and radiation provided the neoplasm has not invaded deeper structures.
Giant cell tumour (GCT) of bone may be a benign aggressive bone lesion with vital recurrence rates following surgical operation.
Historically, these tumors were approached by acting an intralesional curettage of the tumoral tissue by filling the ensuing cavity victimisation morselized os bone autograft.
The main issues of this medical care were the high recurrence rates of up to 40–50%.
Operation with liquid nitrogen as adjuvant therapy for surgical intralesional bone giant cell tumor (GCT) surgery provided encouraging results concerning the recurrence rate and tumor control.
Complication rates in cases were low; adequate exposure, meticulous curettage and burr drilling of the tumoral walls, careful protection of the encompassing soft tissues throughout freeze–thaw cycles and therefore the following reconstruction of the resected region using polymethyl methacrylate and internal fixation especially in weight-bearing areas were essential for a low recurrence rate and a decent practical result.
| Region | Possible side effects |
|---|---|
| cervical carcinoma | It can cause cramping, pain, or bleeding |
| Skin cancer | scarring and swelling. If nerves are damaged, loss of sensation may occur, and rarely, it may cause a loss of pigmentation and loss of hair in the treated area. |
| Bone tumors | destruction of nearby bone tissue and result in fractures, but these effects may not be seen for some time after the initial treatment and can often be delayed with different treatments |
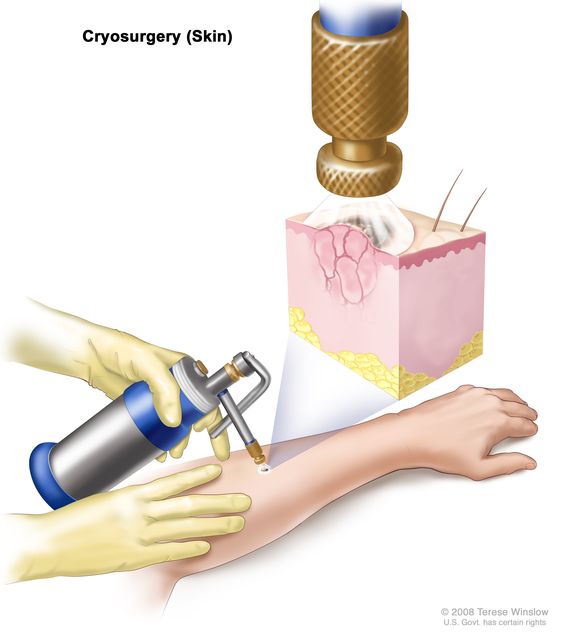
Photo credit: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/cryosurgery
CRYOSURGERY IN GINGIVAL PIGMENTATION
Gingival pigmentation doesn't indicate a medical problem, “black gums” might cause complaints concerning esthetic problems, notably in patients with a high smile line.
Melanin pigmentation may be treated by varied strategies that embody
chemical methods using
- Phenol
- Alcohol
- Ascorbic acid
Surgical methods of
- Depigmentation corresponding to gingival abrasion technique
- Split-thickness epithelial excision
- Gingival abrasion and split-thickness epithelial excision
- Free gingival grafting.
Newer method are
- Cryosurgery
- Laser
- Radiosurgery
Gingival pigmentation occurs as a diffuse, deep-purplish discoloration or as irregularly-shaped brown and light brown patches.
Liquid CO2 remains a usually used cryogen. simple methods, such as direct application to the gums with a cotton wool bud (open), and/or use of expensive probes (closed), are tried with a fair little bit of success in dentistry.
The use of cryogen tetrafluoroethane (TFE) is easy, practical, and cheap as compared to lasers and different standard strategies corresponding to surgical scalpel or chemical methods.
TFE will effectively destroy the gingival epithelium with no damage to the underlying connective tissue and clinically the results were a lot satisfactory with the color, healing, and longevity of the results.

Gingival pigmentation
Photo credit: Drsomitjain (Wikimedia Commons)
CRYOTHERAPY IN OBESITY
The growing prevalence of obesity and overweight is an increase in BMI leads to deposition of sub visceral fat in obesity is related to increased risk of critical conditions together with
- Cardiovascular disease
- Diabetes
- Metabolic syndrome, and a few sorts of cancer.
Body cooling involves either environmental cold exposure or devices to reduce the skin temperature, resulting in systemic or local exposure of fatty tissues to active cooling.
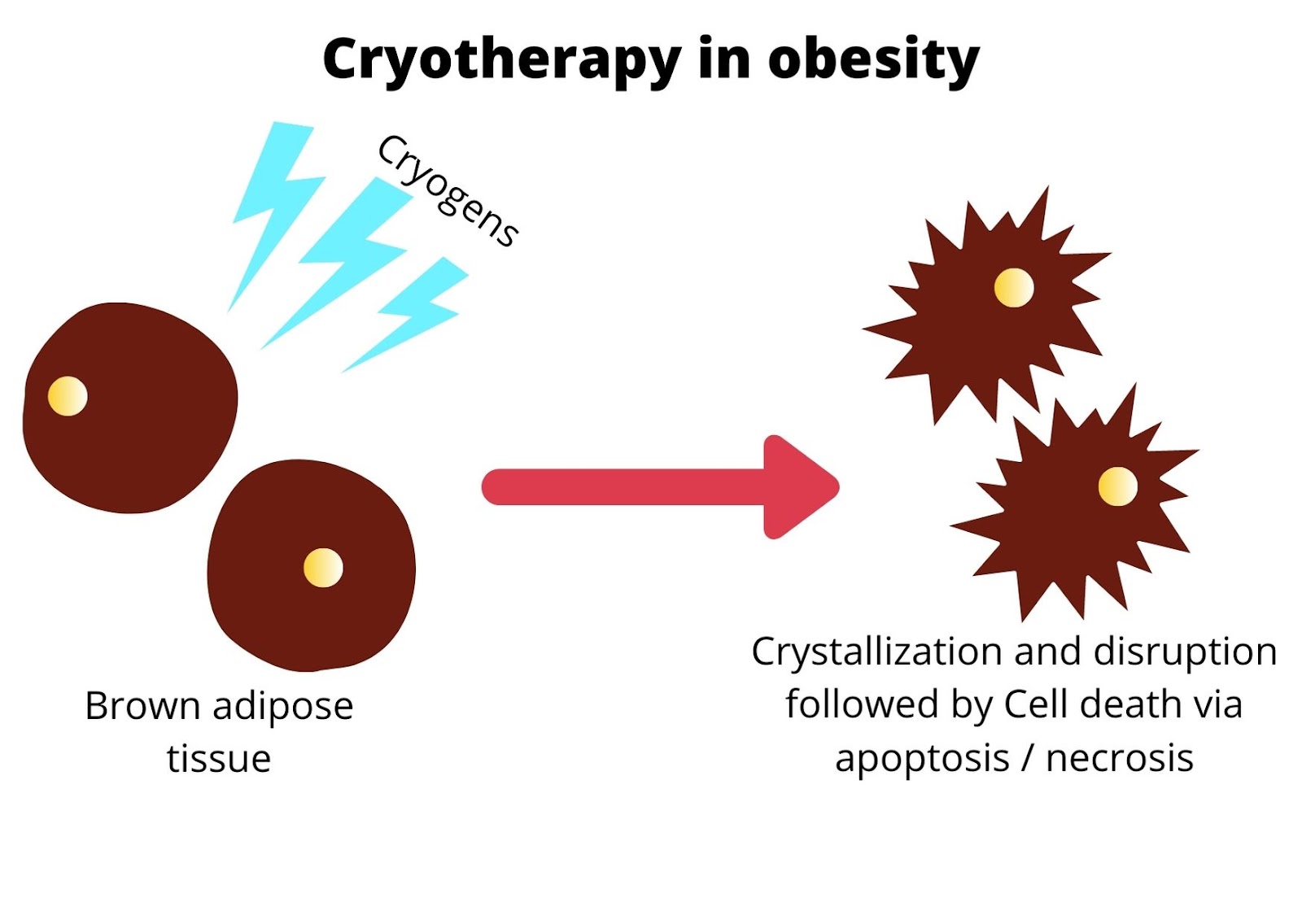
With regard to tissue cooling, it's been hypothesized that adipocytes are more sensitive to cooling than other tissue varieties which cooling leads to
- Crystallization of cytoplasmic lipids
- Disruption of cellular integrity
- Cell death via apoptosis/necrosis
- Inflammation
- Resulting in selective loss of AT
over a amount of weeks to months by a process dubbed “selective cryolysis” or “cryolipolysis”.
A competing hypothesis is that cold exposure would possibly act by boosting energy expenditure via fat metabolism and thermogenesis, leading to reduction of fat mass while not cell disruption.
Two forms of AT are present in humans such as
- White adipose tissue (WAT)
- Brown adipose tissue (BAT).
White adipocytes store excess energy as lipid and function to manage systemic energy balance through the discharge of adipokines that target peripheral tissues and conjointly target the brain to modulate appetite in response to excess energy supply.
Black adipocytes depots will expand in each rate and cell range to take care of the body temperature in response to cooling.
By triggering BAT lipolysis and thermogenesis, cold exposure can scale back the body pool of fatty acids, and prolonged cold exposure can induce the proliferation and differentiation of precursors, resulting in a rise in brown adipocyte numbers.
Cold exposure induces speedy triglyceride uptake from the blood, and fatty triglyceride enzyme activity is instrumental in BAT fat mobilization.
Despite the main focus on BAT, there's proof that WAT can also contribute to cold-induced thermogenesis.
Two elements to cold-induced AT loss, involving
- Rapid energy expenditure by WAT and/or BAT, followed by
- Slow AT loss as a result of continuing metabolic activity, presumably as well as filling of glycogen stores via fat metabolism
- Within the longer term, probably expedited by adjustive conversion of WAT to BAT.
The benefits of cryotherapy might not be restricted to combating obesity:
- Additionally to reducing measures of obesity through cold-induced fat metabolism
- Cold exposure will have additional helpful effects like promoting high-density lipoprotein turnover and reverse cholesterol transport, with probably protecting effects against arteriosclerosis and heart disease.
CRYOGENS IN PRESERVATION OF SPECIMEN
First stage of cryopreservation, the circulation and respiration of the cryonics subject is mechanically restored, and the subject is administered protective medicines and is rapidly cooled to a temperature between 10°C and 0°C.
The subject's blood is washed out and a significant amount of body water is replaced with a cryoprotectant mixture to prevent ice formation.
The subject is cooled to a temperature below −120°C and held in cryostasis.
When and if future medicine has the capability, the subject will be rewarmed, the cryoprotectant will be removed, tissues will be repaired, diseases will be cured, and the subject will be rejuvenated.
Tissues that are vitrified and cryopreserved are assessed for viability moreover as for ultrastructure.
Intracellular K+/Na+ ratio may be an ordinarily used methodology of assessing viability, though different ways (such as measuring of intracellular adenosine triphosphate content) can be helpful within the future.
The Na pump, that maintains membrane potential, won't perform while not binding to ATP and Na+ inside the membrane and K+ outside the membrane.
Though a cell will maintain a membrane potential for many hours without a functional sodium pump, the slow leak of Na+ into the cell and ensuant leak of K+ out of the cell can end in an entire loss of membrane potential once many hours.
Similarly, if the cell dies within the sense of now not being capable of manufacturing energy (ATP) in the mitochondria, the Na pump can stop to operate.
Thus, traditional intracellular K+/Na+ ratios indicate functioning sodium pumps and intact cell membranes.
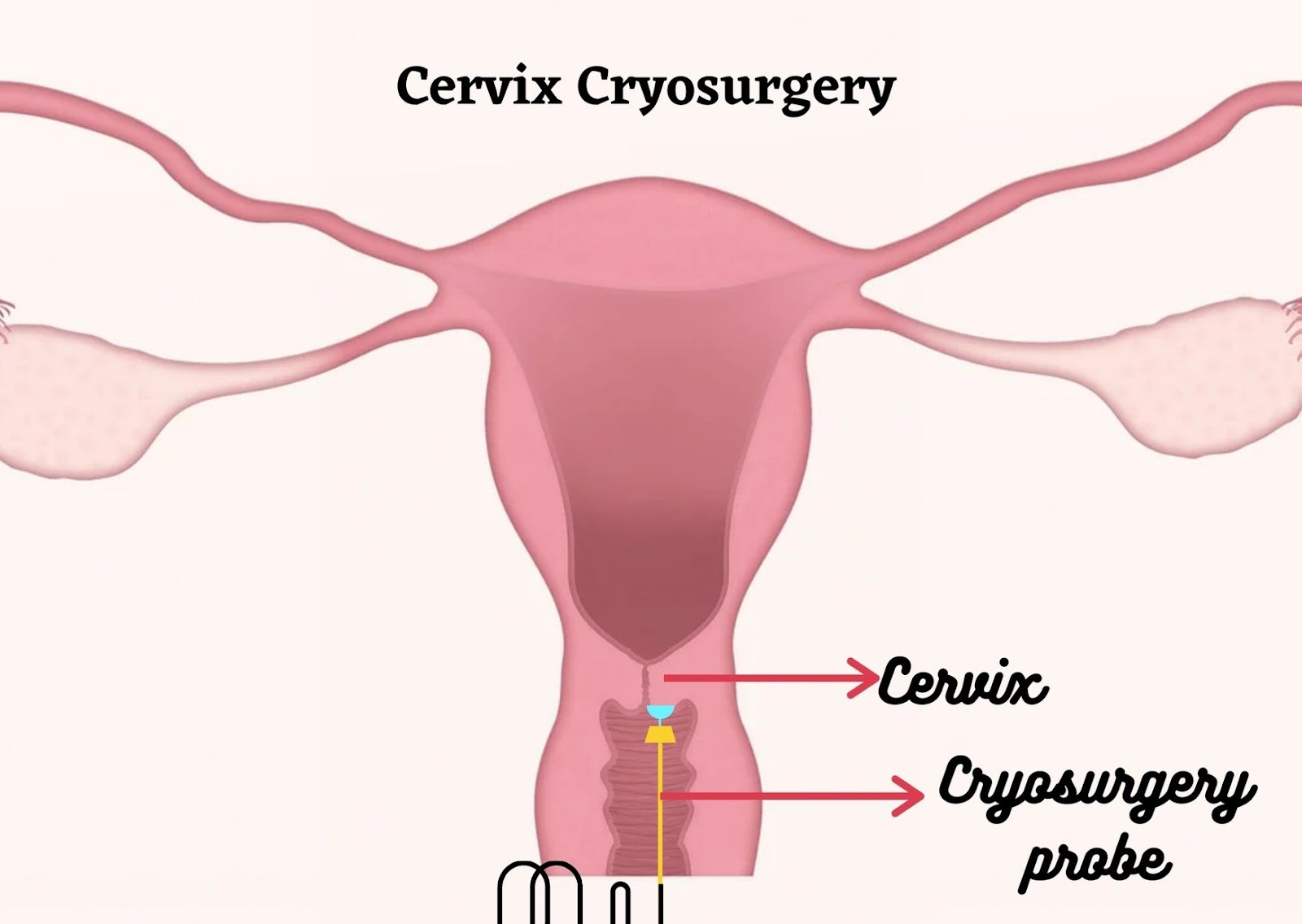
CERVICAL CRYOSURGERY
Cervical ectopy (CE) is related to chronic or repeated symptoms of redness like leucorrhea, vaginal itching or pruritus, dyspareunia, girdle pain, and post-coital bleeding.
CE is distinguished by an erythroderma and inflamed-like region at the external ostium, that forms due to the eversion of the endocervical columnar tissue layer towards the outside.
Cryotherapy may be silent and asymptomatic. If symptomatic, it will cause prolonged physical and psychological distress for girls due to chronic or recurrent discharge and discomfort.
Cryotherapy has a suitable long impact on the treatment of those patients whereas lacking outstanding aspect effects.
Cryotherapy had the very best efficaciousness for reducing abundant leucorrhoea, however the lowest success rate for patients with abundant leucorrhea and repeated cervicitis.
Cryotherapy has some disadvantages, comparatively.
Cauterization wants some precautions; it's the danger of burning lesions if the safeguard plate isn't settled correctly, and it can not be utilized in people with metal prosthetic devices.
Another disadvantage is stricture of the cervix, which has been declared for cauterization over cryotherapy, has not been proved by evidence-based documents.
CONCLUSION
Cryosurgery may be a terribly safe, simple to perform, and comparatively inexpensive technique for treating various oral lesions in an out-patient clinic.
It's an atraumatic variety of therapy as compared to conventional surgery.
Large randomised controlled trials are required before cryotherapy has a longtime role within the management of various diseases.
Hence future research is needed to establish the effectiveness of cryotherapy.
REFERENCE
- Asrani S, Reddy PB, Dhirawani RB, Jain S, Pathak S, Asati P. Cryosurgery: A Simple Tool to Address Oral Lesions. Contemp Clin Dent. 2018;9(Suppl 1):S17-S22. doi:10.4103/ccd.ccd_708_17.
- Narayankar SD, Deshpande NC, Dave DH, Thakkar DJ. Comparative Evaluation of Gingival Depigmentation by Tetrafluroethane Cryosurgery and Surgical Scalpel Technique. A Randomized Clinical Study. Contemp Clin Dent. 2017;8(1):90-95. doi:10.4103/ccd.ccd_1017_16.
- Best BP. Scientific justification of cryonics practice. Rejuvenation Res. 2008;11(2):493-503. doi:10.1089/rej.2008.0661.
- Lal P, Thota PN. Cryotherapy in the management of premalignant and malignant conditions of the esophagus. World J Gastroenterol. 2018;24(43):4862-4869. doi:10.3748/wjg.v24.i43.4862.
- Daugėlaitė, G.; Užkuraitytė, K.; Jagelavičienė, E.; Filipauskas, A. Prevention and Treatment of Chemotherapy and Radiotherapy Induced Oral Mucositis. Medicina 2019, 55, 25.
- Faur, Cosmin & Abu-Awwad, Ahmed & Laurent, Daniel & Pop, Iu & Carmen, Zamfir & Gurgus, Daniela & Hoinoiu, Teodora & Motoc, Andrei & Haivas, Carmen & Grigoras, Mirela & Folescu, Roxana. (2020). Liquid Nitrogen Efficiency in Treatment of Giant Cell Tumor of Bone and Prevention of Recurrence. 10.3390/app10186310.
- Cryosurgery in Cancer Treatment
- Bansal A, Jain S, Gupta S. Cryosurgery in the treatment of oro-facial lesions. Indian J Dent Res 2012;23:297.
- Pedro Thalles Bernardo de Carvalho Nogueira, Mariana Maria Castro Jatobá Remigio, Andreza Maria Correia de Queiroz, Andréia Aparecida da Silva, José Rodrigues Laureano Filho, "Cryosurgery as an Option for the Treatment of Vascular Lesions of the Oral Cavity", Case Reports in Otolaryngology, vol. 2017, Article ID 8529016, 5 pages, 2017. https://doi.org/10.1155/2017/8529016.
- Loap S, Lathe R. Mechanism Underlying Tissue Cryotherapy to Combat Obesity/Overweight: Triggering Thermogenesis. J Obes. 2018;2018:5789647. Published 2018 May 2. doi:10.1155/2018/5789647.
- Abdo J, Cornell DL, Mittal SK and Agrawal DK (2018) Immunotherapy Plus Cryotherapy: Potential Augmented Abscopal Effect for Advanced Cancers. Front. Oncol. 8:85. doi: 10.3389/fonc.2018.00085.
- Agah J, Sharifzadeh M, Hosseinzadeh A. Cryotherapy as a Method for Relieving Symptoms of Cervical Ectopy: A Randomized Clinical Trial. Oman Med J. 2019;34(4):322-326. doi:10.5001/omj.2019.63.









{kind=link}
0 Comments