

INTRODUCTION
Periodontal disease could be a chronic damaging disease that happens in adults, youngsters and children.
Periodontal pathogens which are found within the dental biofilm cause gingival inflammation (gingivitis).
Periodontal diseases are polymicrobial chronic inflammatory diseases that cause the injury of the periodontal ligaments and collapse of the adjacent alveolar bone.
Different factors comparable to
Dental calculus
Overhang restorations
Tooth position
Smoking
Nutrition
Diabetes mellitus
Blood dyscrasia
Age
Genetic alterations
are thought of as predisposing factors of periodontal disease.
Periodontal diseases have several stages starting from delicate and temporary gingivitis to severe periodontitis, which develops once persistent inflammation.
Infections caused by periodontal pathogens like
Porphyromonas gingivalis
Actinobacillus actinomycetemcomitans
Treponema denticola
Tannerella forsythensis
are contributed for periodontitis.
In recent years, there's raised interests in exploring the connection between disease and cancer risk, notably for cancers within the head and neck, upper gastrointestinal system, lung, and pancreas.

POSSIBLE MECHANISM BY WHICH PERIODONTITIS WHICH CAUSE CANCER
Chronic inflammation will induce cell proliferation and mitogenic activities via the activation of signal pathways resembling MAPK/ ERK.
Chronic inflammation can inhibit programmed cell death by modulation of the expression of Bcl- 2 family.
It is planned that persistent infections are able to induce deoxyribonucleic acid injury in proliferating cells through the assembly of toxic substances such as reactive oxygen species (ROS) and reactive nitrogen intermediates (RNI) by inflammatory cells.
Consequently, tissue regeneration leads to DNA damage and permanent genomic alterations in proliferating cells.
Cytokines and chemokines have essential roles in tumour initiation and progression.
Activation of pro-inflammatory cytokines such as IL-6, IL- 8, IL-1β, and TNF-α has been incontestable in cancers.
Microorganisms can induce cancer growth through completely different pathways.
Bacteria manufacture different mediators that promote cell proliferation, mutagenesis and angiogenesis.
Additionally, bacteria inhibit cellular apoptosis.
P. gingivalis is capable of invading and penetrating different epithelial cells which allows it to change some genes in response to chronic infection.
A very recent investigation has demonstrated that P. gingivalis penetrates oral membranes by targeting Grainyhead-like 2 (GRHL2), an epithelial specific transcription factor.
Later, GRHL2 causes epithelial barrier injury by inhibition of tight junction protein expression which ends up in magnified periodontal tissue destruction.
Macrophages are one in every of the foremost necessary inflammatory cells which have important roles in the host innate response to periodontal pathogens.
M1 macrophages promote host immune defense and digest completely different teams of microorganisms, at the same time may cause tissue damage.
M2 macrophages promote tumour development by manufacturing IL- 10, IL-13 and TGF-β. salivary matrix metalloproteinase-8 (MMP8) is higher in patients with disease and might be used as a biomarker for periodontitis.
Autophagy, an intracellular catabolic process, includes a nice impact on cellular homeostasis via the elimination of the damaged organelles and aggregative intracellular proteins.
Compared with healthy periodontal status, the next level of autophagy activity has been found in periodontitis.
It's been proven that autophagy protects periodontal cells from apoptosis, promotes maturation and facilitates oral bacterium to escape from the host’s responses.
LUNG CANCER
Lung cancer is that cancer of the best morbidity and mortality worldwide that still have a poor prognosis even when effective treatment.
Chronic inflammation caused by periodontal microorganism infections, disease may increase the degree of C-reactive protein, IL-6, IFN-γ, and IL-1β .
Periodontal pathogens and inflammation products entered into the bloodstream, which cause general inflammatory response. Indeed, many studies have confirmed that top levels of C-reactive protein, IL-6, IFN-γ, and IL-1β were absolutely related to carcinoma risk.
Pneumonia caused by aspiration of oral bacteria could also be another necessary mechanism.
Many studies have reported a positive relationship between respiratory disease and lung cancer risk .
Understandably, as a clinical indicator of periodontal disease, tooth loss may replicate the degree of poor oral health and was related to carcinoma risk, with a linear relationship.
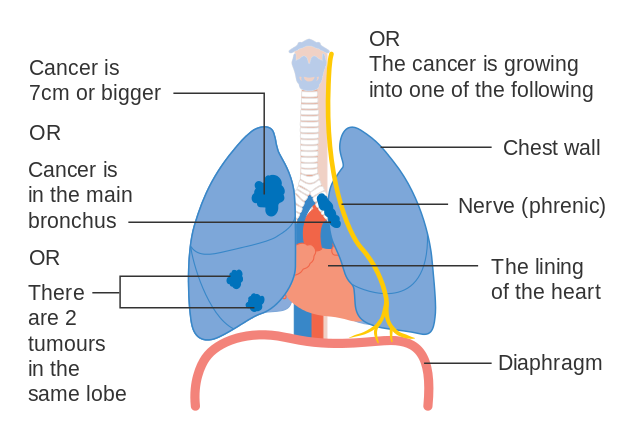
Photo credit: Cancer Research UK (Wikimedia Commons)
BREAST CANCER
One of those mechanisms is primarily based totally at the potential consequences of the inflammatory phenomenon of periodontitis at the systemic dissemination of the locally produced mediators, together with C-reactive protein (CRP), interleukins-1 beta (IL-1β) and -6 (IL-6), and tumor necrosis factor-alpha (TNF-α).
Study in Sweden said that the continual periodontal disease indicated by way of means of lacking molars regarded to accomplice statistically with breast cancer.
Chronic gum sickness or had misplaced teeth because of periodontal sickness have been located to be greater than instances as possibly to be identified with breast cancer compared to individuals who had healthful gums.
The byproducts of the oral inflammation enter the bloodstream, which might also additionally enhance cell proliferation and mutagenesis, taking into account the development and spread of cancer.

COLORECTAL CANCER
Colorectal carcinoma (CC) is the fourth cause of Malignant neoplasm deaths, responsible for just about 610,000 deaths per annum worldwide.
CC is one in all the primary and best genetically characterized Malignant tumours, and specific somatic mutations in oncogenes and tumour suppressor genes are found that are related to progression from adenomatous lesions (polyps) to invasive MTs.
A. actinomycetemcomitans and gastric precancerous lesions appreciate chronic atrophic gastritis, intestinal metaplasia, or dysplasia had been indicated.
Patients with esophageal cancer,
Treponema denticola
Streptococcus mitis
Streptococcus anginosus
are the most microorganisms, however, Fusobacterium nucleatum is the main part of oral microbiome within the patients with large intestine cancer.
In addition, P. gingivalis and the Fusobacterium species have been found in esophageal cancer, large intestine cancer and pancreatic cancer.
Fusobacterium nucleatum, a gram-negative anaerobe, to be extremely enriched in CC.
Fusobacterium nucleatum is found in high microorganism loading in periodontal disease. FadA (Fusobacterium adhesin A) adhesion of FN aroused human CC cell growth.
FadA binds vascular endothelial-cadherin on endothelial cells, inflicting raised endothelial cell permeability therefore permitting bacteria to penetrate, a possible mechanism employed by FN for general dissemination.
F. nucleatum binds to and invades each normal and MTs epithelial cells via FadA binding to epithelial (E)-cadherin.
This binding ends up in growth stimulation of human CC cells however not the non-cancerous cells. FadA binding to E-cadherin on MTs cells activates b-catenin-regulated transcription, leading to raised expression of oncogenes cyclin D1 and c-Myc, Wnt (wingless-related integration site) signalling genes Wnt7a, Wnt7b, and Wnt9a, and inflammatory genes nuclear factor-k B, interleukin-6 (IL-6), IL-8, and IL-18, all of that are hallmarks of carcinogenesis.
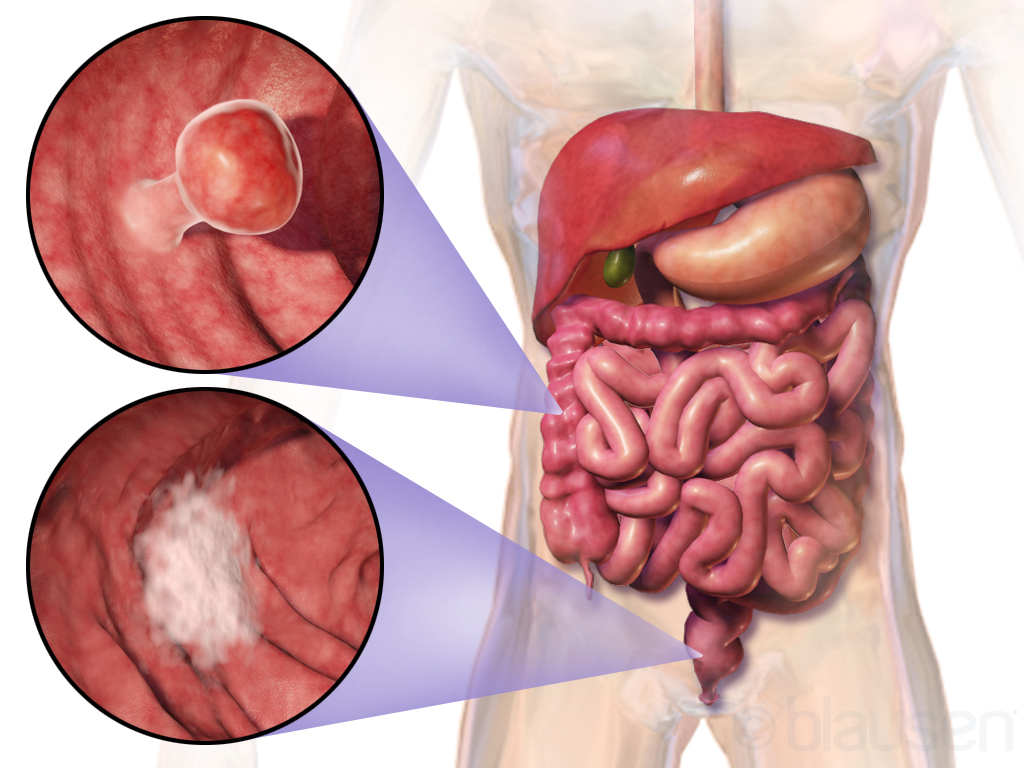
Photo credit: Blausen Medical Communications, Inc., (Wikimedia Commons)
PROSTATE CANCER
Prostate cancer is the most frequent cancer to occur in males and second foremost reason behind cancer-related death within the Western world.
Prostate cancer is of serious concern because of the gradual increase in the variety of aging men and therefore the existence of quite three million men with the disease.
Recent observations counsel that prostatic adenocarcinoma is related to chronic inflammation.
Reports suggest that periodontitis is considerably associated with an accrued risk of prostate cancer.
Periodontal pathogens could also be migrating through the circulation to initiate an infection and inflammatory response in the prostate.
The prostate inflammatory responses might in turn induce neoplastic transformations.
Prostate-specific antigen (PSA) levels as a marker of inflammation in patients with prostatitis associated periodontal disease and showed that subjects with each disease have larger levels of PSA.
Presence of inflammatory cell infiltrates and proliferative inflammatory atrophy (PIA) are usually detected in histological samples of benign and malignant prostates.
PIA is an inflammatory lesion rising as a result of infection or cell injury ulterior from radical toxicity, hypoxia, infection or autoimmunity.
These lesions might result in malignancy through an accumulation of transmutation in quickly dividing cells.
Proliferative inflammatory atrophy is perhaps a precursor lesion to cancer and regularly exists near to high-grade prostatic intraepithelial neoplasia (HGPIN) or early cancer.
It's been determined that a genetic association between PIA, HGPIN, and cancer exists.
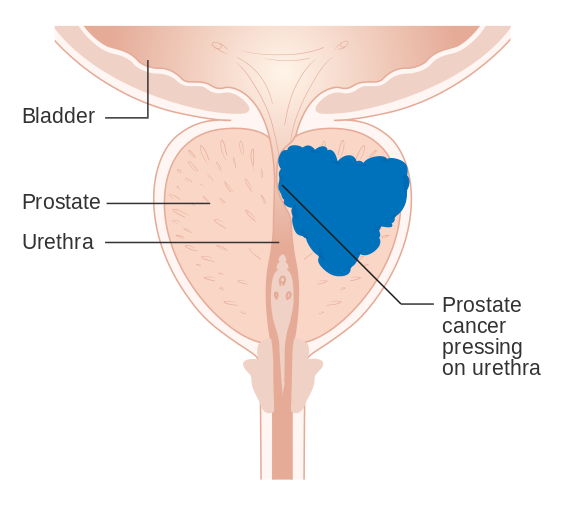
Prostate cancer: Cancer Research UK (Wikimedia Commons)
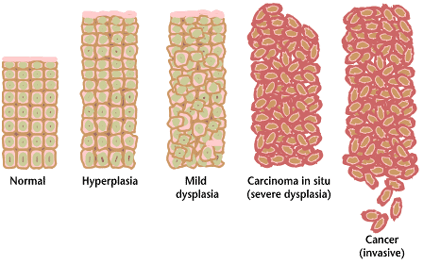
ORAL CANCER
Squamous cell carcinoma is the most frequent malignancy within the oral cavity and with nearly 4,00,000 new diagnosed patients worldwide every year; it represents the sixth frequent malignant tumour.
Oral membrane undergoes completely different developmental stages from hyperkeratosis over different degrees of abnormalcy to invasive cancer, whereas each level shows consecutive incidental to alterations inside the genetic profile.
Chronic periodontal disease acts as a promoter for the invasion of tumor cells into the bone.
During the course of chronic periodontitis, the loss of clinical attachment level and therefore the underlying bone is well triggered.
The periodontal-localized inflammation macerates the cellular bone by increased osteoclastic activity which can constitute a possible route for invasion of an adjacent carcinoma.
Alveolar squamous cell carcinomas being directly associated with teeth that show extensive signs of chronic periodontal disease.
Clinical sign for chronic periodontitis being an independent risk issue for the event of carcinoma within the oral cavity.

Photo credit: Welleschik (Wikimedia Commons)
CONCLUSION
Periodontitis could be a common illness round the world.
Oral microbiome is the main borne factor for periodontal diseases.
Inflammatory responses will increase the chance of genetic alterations and malignant transformation.
Doctors ought to think that patients with periodontitis are joined to a multiplied risk of various cancers.
Education and training of oral health practitioners can scale back the implications of each periodontitis and various cancers.
Periodontal disease will be thought-about as a risk considering cancer however further studies are required to clarify these suggested associations.
REFERENCE
- Sadighi Shamami M, Sadighi Shamami M, Amini S. Periodontal Disease and Tooth Loss as Risks for Cancer: A Systematic Review of the Literature.Iran J Cancer Prev. 2011;4(4):189-198.
- You Chen, Bao-ling Zhu, Cong-cong Wu, Rui-fang Lin, Xi Zhang, "Periodontal Disease and Tooth Loss Are Associated with Lung Cancer Risk", BioMed Research International, vol. 2020, Article ID 5107696, 12 pages, 2020. https://doi.org/10.1155/2020/5107696.
- Irani S, Barati I, Badiei M. Periodontitis and oral cancer - current concepts of the etiopathogenesis.Oncol Rev. 2020;14(1):465. Published 2020 Mar 18. doi:10.4081/oncol.2020.465.
- Saini R. Oral health links breast cancer. J Pharm Bioallied Sci. 2011;3(3):468. doi:10.4103/0975-7406.84473.
- Lauritano D, Sbordone L, Nardone M, Iapichino A, Scapoli L, Carinci F. Focus on periodontal disease and colorectal carcinoma. Oral Implantol (Rome). 2017;10(3):229-233. Published 2017 Nov 30. doi:10.11138/orl/2017.10.3.229.
- da Silva APB, Alluri LSC, Bissada NF, Gupta S. Association between oral pathogens and prostate cancer: building the relationship. Am J Clin Exp Urol. 2019;7(1):1-10. Published 2019 Feb 18.









0 Comments