

INTRODUCTION
Blood may be a special style of connective tissue that's composed of
- white cells
- Red cells
- Platelets and
- Plasma.
it's a range of functions within the body.
Plasma is that the extracellular material created from water, salts, and various proteins that, beside platelets, encourages blood to clot.
Proteins in the plasma react with air and harden to stop more bleeding.
The white blood cells are accountable for the immune defense.
They search out invading organisms or materials and minimize their result in the body.
Being alive is not possible while not blood, the complex liquid containing legion chemicals and cells.
Increase in the number of surgical procedures (both elective and emergency) and trauma cases, the demand for human blood for transfusion has seen an overwhelming rise.
The quantity of units collected from blood donors is low to cope up with the increasing needs of human blood that modern-day medication and surgery demands.
Additionally, given human blood is fraught with considerations involving short storage life, chance of transmission of blood borne infections, aversions and increasing prices of collecting, process and crossmatching.
To mitigate this ever increasing inequality between the demand and supply of blood and therefore the difficulties related to keeping human blood, artificial blood has emerged as a promising option.

ARTIFICIAL BLOOD
Artificial blood could be a product made to act as a substitute for red blood cells.
Artificial blood was highlighted once emergence of HIV in 1980 due to the chance of its transmission by blood transfusion, which imposes higher prices due to the required detection tests.
Some of the ideal artificial blood products should have the subsequent characteristics.
- It should be safe to use and compatible inside the human body. This implies that completely different blood types shouldn't matter when a synthetic blood is used. It conjointly implies that artificial blood will be processed to get rid of all disease-causing agents reminiscent of viruses and microorganisms.
- It should be shelf stable. unlike to|not like} given blood, liquid will be kept for over a year or more. This can be in contrast to natural blood which may solely be stored for one month before it breaks down.
- It must be ready to transport elements throughout the body and unharness it wherever it's needed.
Photo credit: BruceBlaus (Wikimedia Commons)
HISTORICAL EVENTS IN THE DEVELOPMENT OF ARTIFICIAL BLOOD
| Year | Event |
|---|---|
| Sixteenth century | Scientific practitioners attempted numerous materials which include beer, urine, milk, plant resins, and sheep blood alternatively for blood. |
| 1667 | The first a success human blood transfusions had been achieved. Unfortunately, the practice become halted due to the fact patients who acquired next transfusions died. |
| 1854 | Patients had been injected with milk to deal with Asiatic cholera. Physicians believed that the milk helped regenerate white blood cells. |
| 1883 | Improvement of synthetic blood got with the introduction of Ringer's solution—a solution composed of sodium, potassium, and calcium salts. |
| 1871 | Resercher had tested using animal plasma and blood instead for human blood. |
| 18th century | Research of Landsteiner in the diverse blood groups, blood transfusion have become a more secure and mounted clinical procedure. |
| 1920s | Research advised that this gum-saline solution containing galactoso-gluconic acid turned into used to increase plasma had a few negative health effects |
| 1930 | Using this gum solution had considerably diminished |
| 1947 | Established order of blood banks via way of means of the American Red Cross |
| 1966 | Experiments with mice advised a brand new kind of blood substitute, perfluorochemicals (PFC). |
PERFLUROCARBONs
The ability for perfluorocarbons (PFCs) to be used as oxygen carrying agents was 1st delineated by Clark and Gollan in 1966.
Perfluorocarbons are chemically inert molecules with structural similarity to hydrocarbons and wherever the H groups are replaced with fluorine.
PFC are biologically inert materials that may dissolve regarding fifty times a lot of oxygen than blood plasma.
They're comparatively cheap to provide and may be created barren of any biological materials.
This eliminates the important chance of spreading an communicable disease via a blood transfusion.
Oxygen is dissolved in PFCs at a level of about 40%–50%, that is twenty times on top of the capacity of water and a couple of times on top of plasma.
In addition, fluorocarbons dissolve 130–160 milliliter carbon dioxide, that is 2 to 3 times higher than the corresponding water capability.
PFCs are not soluble in water, hence they have to be blended by addition of lipids through high homogenisation which suspends little particles of PFC within the blood.
PFCs are heat resistant and may stand up to 300°C and better temperatures with none change, which makes them simply amenable to heat sterilization.
PFC’s are classified as
- First Generation PFC: Fluosol DA 20% was the model of this class and consisted of perfluorodecalin and perfluoro tripropylamine.
- Second Generation PFC: Perfluorodecalin, perfluorooctyl bromide and bis (perfluorobutyl) ethylene belong to the present class.
Fluosol, as mentioned above, incontestable this “proof of principle” that led to a more modern formulation being Food and Drug Administration approved in 1989, however it eventually suffered from clinical shortcomings.
PFC products can't be utilized by the human body and needs to be removed and this method needs around 18-24 months.
They'll overload the reticuloendothelial system and suppress its function. because it will be maintained in organs, histologic effects like appearances and enlargement of cavity histiocytes are seen in liver biopsies.
Administration of PFC-based products may end up in delicate thrombocytopenia (10%–15% reduction in blood platelet count) as well as flu-like syndrome.
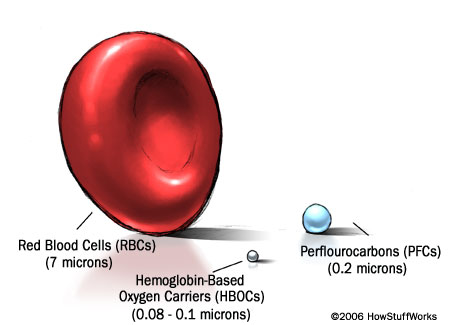
Photo credit: Howstuffworks
HAEMOGLOBIN BASED OXYGEN SUBSTITUTES
Hemoglobin carries oxygen from the lungs to the other tissues within the body.
Artificial blood supported Hb takes advantage of this natural function.
Human Hb derived from terminated red blood cell bags is the main supply of Hb for the assembly of Hb-based RBC substitutes.
Raw hemoglobin can't be used as a result of it might break down into smaller, hepatotoxic compounds among the body.
There also are issues with the steadiness of hemoglobin in a solution.
The challenge in making a hemoglobin-based artificial blood is to change the hemoglobin molecule so these problems are resolved.
Cell-free hemoglobin will doubtless be used as a blood substitute because hemoglobin maintains its ability to move O2 outside of the RBC; however, unfortunately, it's quite hepatotoxic to close tissues.
Toxicity includes epithelium scavenging of nitric oxide (NO) that ends up in narrowing of the blood vessels and also the development of O2-, heme-, and globin-based radicals.
Haemoglobin based oxygen carriers (HBOC) are classified as
- The 1st generation of blood substitutes to be created were the stroma-free hemoglobin (SFH) products. SFHs were ready by lysis of packed RBCs forming soluble hemoglobin. This mixture was then centrifuged to get rid of the majority of red cell stroma, resulting in the assembly of SFH.
- The second-generation HBOCs were pyridoxilated hemoglobin-polyoxyethylene conju-gates (PHPCs) that are prepared through chemical modification of SFH. These products are designed to stop the most important disadvantages of SFHs reported in multiple studies, namely, increased O2 affinity, short circulatory half-life, and nephrotoxicity.
- The third-generation blood substitutes embrace Hb crosslinked between the α chains with bis(dibromosalicylic) fumarate (DBBF) or αα-hemoglobin.
Sometimes, bovine blood has got to be used for acquisition of haemoglobin.
Bovine haemoglobin has the potential of harbouring the particle microorganism to blame for inflicting bovine spongiform encephalopathy.
HBOC circulation half life is shorter than traditional RBCs.
Majority of HBOC stay in circulation for around 20-30 hours whereas blood transfusion lasts thirty four days.
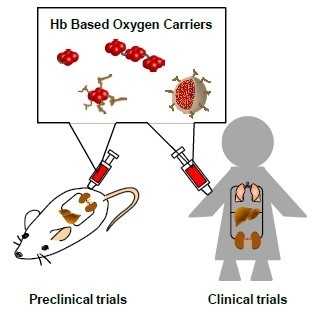
Photo credit: Taguchi, K.; Yamasaki, K.; Maruyama, T.; Otagiri, M. Comparison of the Pharmacokinetic Properties of Hemoglobin-Based Oxygen Carriers. J. Funct. Biomater. 2017, 8, 11. https://doi.org/10.3390/jfb8010011
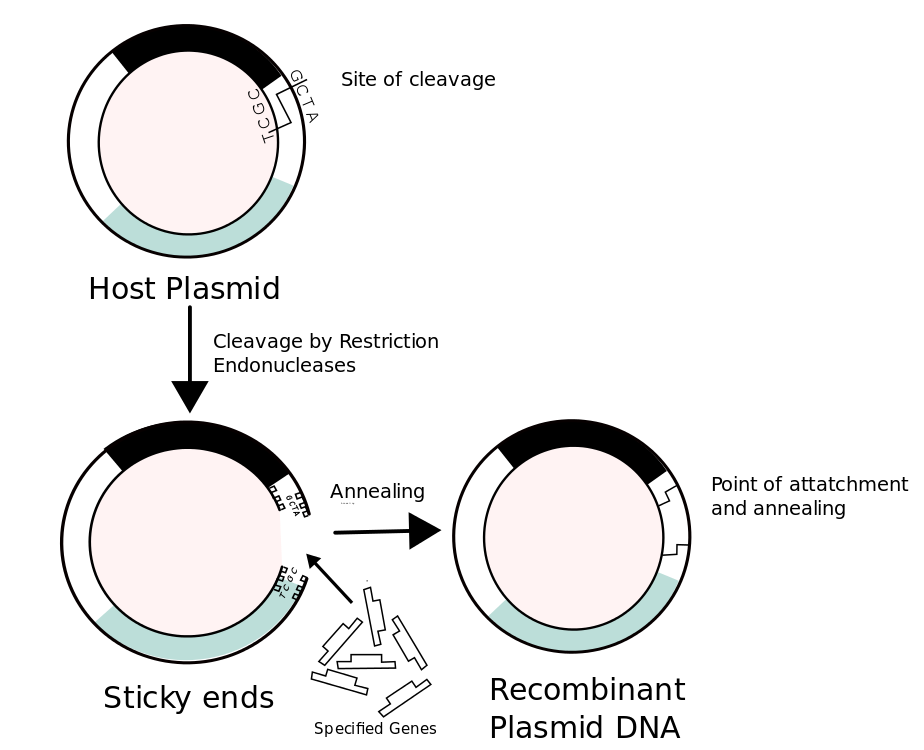
RECOMBINANT HAEMOGLOBIN
INITIAL STEP
Recombinant DNA technologies is utilised to supply changed haemoglobin in organisms like E.coli and yeast.
A strain of E. coli bacteria that has the power to produce human hemoglobin is used. Over the course of about 3 days, the protein is harvested and therefore the microorganisms are destroyed.
To begin the fermentation process, a sample of the pure bacteria culture is transferred to a test tube that contains all the nutrients necessary for growth.
This first inoculation causes the bacteria to multiply.
Once the population is nice enough, they're transferred to a seed tank.
STEP 2
A seed tank could be a massive stainless-steel kettle that has an ideal atmosphere for growing microorganisms. It's stuffed with heat water, food, and an ammonia supply that are all needed for the assembly of hemoglobin.
Different growth factors corresponding to vitamins, amino acids, and minor nutrients are added.
The microorganism solution within the seed tank is constantly bathed with compressed gas and mixed to stay it moving.
Once enough time has passed, the contents of the seed tank is wired to the fermentation tank.
STEP 3
The fermentation tank could be a larger version of the seed tank.
It's also filled with a growth media required for the bacteria to grow and turn out Hb.
Since pH control is significant for best growth, liquid is added to the tank as necessary.
Once enough hemoglobin has been produced, the tank is empty thus isolation can begin.
STEP 4
Isolation begins with a centrifugal centrifuge that isolates a lot of the hemoglobin.
It will be further segregated and sublimate victimization divisional distillation.
This commonplace column separation method relies on the principle of boiling a liquid to separate one or more parts and utilizes vertical structures referred to as fractionating columns.
From this column, the hemoglobin is transferred to a final process tank.
FINAL STEP
Here, it's mixed with water and different electrolytes to turn out the bogus blood.
The bogus blood will then be pasteurised and placed into an acceptable packaging.
The standard of compounds is checked often throughout the whole process.
Notably vital are frequent checks created on the microorganism culture.
PEGylated HAEMOGLOBIN
polyethylene glycolated (PEG) hemoglobin derived from either human or bovine sources is any change with maleimide or carboxylated to manufacture a haemoglobin with distinctive O2 transport functions.
Hemospan, conjointly mentioned as MP4, could be a human hemoglobin-based agent that was developed to mediate the vasoactivity and hypertensive effects of antecedently developed
PEGylated hemoglobin molecules.
MP4 to be most helpful in things wherever organ tissue PO2 is low and with restricted introduction cherished within the states of shock or traumatic ischemia.
Sanguinate is a PEGylated and carbon monoxide-hybridized (PEG-COHb) OTA with modes of action that will be useful to mitigate the constraints of the earlier generations of HBOCs.
Sanguinate has been granted orphan drug status for treatment of sickle cell disease by the FDA
CONCLUSION
Due to the raised demand for transfusion and issues concerning blood-borne pathogens, development of artificial blood substitutes, particularly HBOCs, is under intensive focus.
The intensive clinical application of those substances is presently obstructed by problems regarding safety, cost, lower intravascular dwell times, comfortable provide of raw materials, toxicity and prolonged tissue retention.
Future analysis initiatives during this context should, therefore, be directed towards providing adequate quantities of safe, efficacious, commercially viable alternatives with lesser drawbacks which are able to cut back dependency on given blood and reduce mortality because of transfusion requirements.
REFERENCE
- Sarkar S. Artificial blood. Indian J Crit Care Med. 2008;12(3):140-144. doi:10.4103/0972-5229.43685.
- Haldar R, Gupta D, Chitranshi S, Singh MK, Sachan S. Artificial Blood: A Futuristic Dimension of Modern Day Transfusion Sciences. Cardiovasc Hematol Agents Med Chem. 2019;17(1):11-16. doi:10.2174/1871525717666190617120045.
- Khan F, Singh K, Friedman MT. Artificial Blood: The History and Current Perspectives of Blood Substitutes. Discoveries (Craiova). 2020;8(1):e104. Published 2020 Mar 18. doi:10.15190/d.2020.1.
- Moradi S, Jahanian-Najafabadi A, Roudkenar MH. Artificial Blood Substitutes: First Steps on the Long Route to Clinical Utility. Clin Med Insights Blood Disord. 2016;9:33-41. Published 2016 Oct 27. doi:10.4137/CMBD.S38461.









0 Comments