

WHAT IS MUCORMYCOSIS OR BLACK FUNGUS?
Mucormycosis is a rare fungal infection that is life-threatening and it is also known as a black fungus. Mucorales are usually seen in the environment which includes soil, bread, decaying vegetable matter and dust. As it causes black lesion because of tissue necrosis it is called a black fungus.
There are numerous medical kinds of mucormycosis infection they're
- Pulmonary mucormycosis
- Rhinocerebral mucormycosis
- Gastrointestinal mucormycosis
- Encephalic mucormycosis
- Cutaneous mucormycosis.
Mucormycosis reveals a marked propensity to invade blood vessels, mainly to thrombosis, tissue necrosis, and infarction of tissue, and mortality is high. The general mortality rate for mucormycosis remains >50%, and it becomes 100% amongst patients with disseminated disease or people with chronic neutropenia.
Thus in this article, we are going to get answers about what is mucormycosis and what its signs and symptoms are and why it is happening in covid patients particularly why it is happening in post covid infection.

Patient with diabetes and immunocompromised having a higher chance of getting Mucormycosis
WHO IS AT RISK OF GETTING MUCORMYCOSIS?
It is mostly affecting patients with
- Diabetes Mellitus (DM)
- Immunocompromised patient
- A patient who is in long term steroid use
- High level of iron in the blood
- The person who had recently organ transplant
- Neutropenia
- Diabetic ketoacidosis
- Carcinoma
- Chronic renal failure
- Acquired immunodeficiency syndrome (AIDS)
Covid 19 is also an important risk factor of getting mucormycosis because of the following reasons Glucocorticoids (steroid) are inexpensive, broadly available, and were proven to lessen mortality in hypoxemic sufferers with COVID-19 alongside with immunomodulatory tablets consisting of tocilizumab (immunosuppression) should similarly increase the chance of infections in COVID-19 sufferers.
HOW THE MUCORMYCOSIS ENTER INTO OUR BODY?
The primary direction of infection is through air spore inhalation, which deposits withinside the paranasal sinuses and the lung which causes rhinocerebral or pulmonary mucormycosis.
Other routes much less regularly encountered result from ingestion or direct pores (wounds) and skin inoculation which causes cutaneous mucormycosis.
HOW THE MUCORMYCOSIS FUNGUS AFFECT OUR BODY (PATHOGENESIS)?
Mucormycosis infection consists of 2 main pathogenesis they are
- IN BLOOD VESSELS
Mucormycosis infections are characterised using tremendous invasion into the blood vessels that result in vessel thrombosis and next tissue necrosis. Damage of and penetration via endothelial cells or the extracellular matrix proteins lining blood vessels is possibly to be a life-threatening level of this fungus.
- MECHANISM OF IRON UPTAKE
Because of the blood invasive nature of this fungus, heme (H) found in RBC is probably to represent a supply of iron to the invading fungus, which both takes up heme intracellularly or strips ferric iron from heme via way of means of the action of the reductase-permease system. If heme is transported intracellularly, ferric iron is received via means of the action of heme oxygenase withinside the cytoplasm.
Patients receiving dialysis who's dealt with with the iron chelator deferoxamine also are uniquely prone to a deadly form of mucormycosis via way of means of Deferoxamine immediately chelates iron from transferrin, ensuing withinside the iron-deferoxamine complex.
PATHOGENESIS IN DIABETIC PATIENTS
Mucormycosis is a well-identified complication of poorly managed Diabetes mellitus that is related to defects in innate immunity, especially chemotaxis, phagocytosis and killing through PMNs, and monocytes/macrophages.
Rhizopus species have an active ketone reductase system, which can be a further virulence element via means of improving growth withinside the acidic and glucose-rich surroundings seen in diabetic ketoacidosis and thereby promoting the growth of the fungus.
Patients with DKA who're uniquely prone to mucormycosis lend aid to the position of iron uptake in the pathogenesis of the disease.
PATHOGENESIS IN COVID PATIENTS
Covid patients with diabetes mellitus, neutropenia, the chronic obstructive pulmonary sickness has given aggressive therapy including corticosteroid therapy, ventilation, intensive care unit stay cause an immunocompromised state which develop extreme opportunistic infections including black fungus.
Alteration of the innate immunity because of COVID-19-related immune dysregulation characterised through reduced T cells, along with CD4 and CD8 cells cause a change withinside the immune system.
The use of steroids (intravenous dexamethasone), monoclonal antibodies, and broad-spectrum antibiotics for the control of COVID-19 infection can increase the probabilities of having mucormycosis.
RHINOCEREBRAL MUCORMYCOSIS
Rhinocerebral mucormycosis is described as a fungal infection concerning the nostril, paranasal sinuses, and mind. Inhalation of spores from fungi residing in soil or natural matter in immunocompromised sufferers is the maximum common course of the invasion of this kind.
The humid surroundings of the nostril and paranasal sinuses favours the boom and invasion of fungi. Invasion of the mind and orbit is through the involvement of sphenopalatine and internal maxillary arteries.
The involvement of the internal carotid artery and cavernous sinus thrombosis is common only in long-status cases.

PULMONARY MUCORMYCOSIS
Pulmonary mucormycosis includes the improvement of bilateral pneumonia, which is swiftly revolutionary and the result of the inhalation of infectious material. Hemoptysis typically takes place with vascular invasion, which could occasionally be deadly. Pulmonary mucormycosis is a hastily fatal illness, with a usual mortality rate of 76%, which will increase to 95% with extrathoracic dissemination.
CUTANEOUS MUCORMYCOSIS
Cutaneous mucormycosis is regularly obtained via means of direct inoculation, surgery, burns, infected dressings, motor automobile accidents, and insulin injection sites.
In healthcare centres, mucormycosis is occurring because of infected adhesive tape, wood tongue depressors, vascular gadgets, nitroglycerine patches, ostomy bags, and building production contamination.
Cutaneous mucormycosis is of sorts; they are primary and secondary. In primary disease, the pores and skin is infected via means of direct inoculation and in secondary disease, via means of dissemination from different locations, extra usually from a rhinocerebral infection.
WHAT ARE THE SYMPTOMS OF MUCORMYCOSIS?
Mucormycosis symptoms of various types include
Signs and symptoms of rhinocerebral black fungus were
- One-sided headache particularly in the back of the eyes
- Nausea
- Nasal congestion
- Facial ache and numbness
- History of black nasal discharge
- Fever
- Epistaxis
- Nasal hypoesthesia
- Rhinorrhea
- Black eschar is seen on nasal mucosa or palatine mucosa
- Diplopia
- Vision loss
- Periorbital ache
- Amaurosis
- Blurring of vision
- Sinusitis
- Dizziness
- Altered intellectual status
- Gait.
signs and symptoms of pulmonary black fungus were
- Bronchitis
- Bronchopneumonia
- Pulmonary embolism
- Fever
- Hemoptysis
- Dyspnea
- Cough.
signs and symptoms of cutaneous black fungus were
- Cellulitis
- Abscesses
- Skin swelling
- Necrosis.

HOW WILL YOU DIAGNOSIS MUCORMYCOSIS?
The mucormycosis diagnosis is difficult and treatment needs to begin as early as possible on the way to lower mortality.
COMPUTER TOMOGRAPHY (MUCORMYCOSIS RADIOLOGY)
Radiological imaging studies are required to analyze regions with suspected mucormycosis, mainly CT withinside the brain, paranasal sinuses, lungs, and abdomen.
Findings withinside the CT scan of the brain and paranasal sinuses covered soft tissue oedema of cavity mucosa, sinus mucoperiosteal thickening, bone erosions, and orbital invasions in case of rhinocerebral mucormycosis.
Findings withinside the CT of the chest protected pleural effusion, nodules, consolidation, and ground-glass infiltrate in case of pulmonary mucormycosis.
BIOPSY
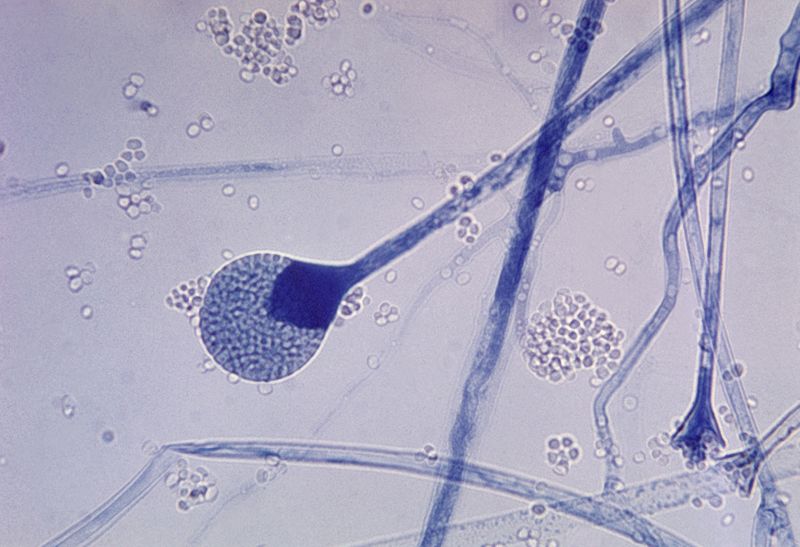
The biopsy needs to be taken from the centre of the lesion. Histology is more beneficial in number one in mucormycosis. Thick, hyaline, non-septated and bifurcated hyphae can be visible with hematoxylin and eosin stain.
WHAT IS THE TREATMENT FOR MUCORMYCOSIS?
MEDICAL TREATMENT
Amphotericin B is taken into consideration first-line remedy for mucormycosis. The lipid method of amphotericin B is run in excessive doses intravenously as soon as a day as a preliminary therapy.
The monitoring of serum electrolytes, creatinine, and urea are done to assess the status of renal function.
Posaconazole has a few proofs as a second-line remedy in mucormycosis. The suggestions do not help the aggregate of amphotericin and posaconazole.
SURGICAL TREATMENT
Surgical elimination of the involved body tissue and fungal increase supervened via way of means of drainage is indicated after drug remedy. Proper clearance of involved tissue needs (>1 cm) excision of healthful tissue is needed to remove the disease.
SUPPORTIVE TREATMENT
Hyperbaric oxygen affords enough oxygen to neutrophils to kill fungi, and rifampicin is the adjuncts to systemic amphotericin B. The extended oxygen stress improves the capacity of neutrophils to kill the organism and enables wound healing.
TREATMENT IN COVID PATIENTS
Along with antifungal pills (amphotericin B), use of glucocorticoids in moderate COVID-19 cases (without hypoxemia) or the usage of higher doses of glucocorticoids need to be avoided and pills focused on immune pathways including tocilizumab need to be discouraged.
REFERENCES
- Ibrahim AS, Spellberg B, Edwards J Jr. Iron acquisition: a novel perspective on mucormycosis pathogenesis and treatment. Curr Opin Infect Dis. 2008;21(6):620-625. doi:10.1097/QCO.0b013e3283165fd1.
- Sarkar, Sandip; Gokhale, Tanmay; Choudhury, Sushmita Sana1; Deb, Amit Kumar COVID-19 and orbital mucormycosis, Indian Journal of Ophthalmology: April 2021 - Volume 69 - Issue 4 - p 1002-1004 DOI: 10.4103/ijo.IJO_3763_20.
- Ibrahim AS, Spellberg B, Walsh TJ, Kontoyiannis DP. Pathogenesis of mucormycosis. Clin Infect Dis. 2012;54 Suppl 1(Suppl 1): S16-S22. doi:10.1093/cid/cir865.
- Wang XM, Guo LC, Xue SL, Chen YB. Pulmonary mucormycosis: A case report and review of the literature. Oncol Lett. 2016;11(5):3049-3053. doi:10.3892/ol.2016.4370.
- Castrejón-Pérez AD, Welsh EC, Miranda I, Ocampo-Candiani J, Welsh O. Cutaneous mucormycosis. An Bras Dermatol. 2017;92(3):304-311. doi:10.1590/abd1806-4841.20176614.
- Skiada A, Lanternier F, Groll AH, et al. Diagnosis and treatment of mucormycosis in patients with haematological malignancies: guidelines from the 3rd European Conference on Infections in Leukemia (ECIL 3). Haematologica. 2013;98(4):492-504. doi:10.3324/haematol.2012.065110.
- Bhandari J, Thada PK, Nagalli S. Rhinocerebral Mucormycosis. [Updated 2020 Nov 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-.
- Hernández JL, Buckley CJ. Mucormycosis. [Updated 2020 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-.
- Camara-Lemarroy CR, González-Moreno EI, Rodríguez-Gutiérrez R, et al. Clinical features and outcome of mucormycosis. Interdiscip Perspect Infect Dis. 2014;2014:562610. doi:10.1155/2014/562610.
- Garg D, Muthu V, Sehgal IS, et al. Coronavirus Disease (Covid-19) Associated Mucormycosis (CAM): Case Report and Systematic Review of Literature. Mycopathologia. 2021;186(2):289-298. doi:10.1007/s11046-021-00528-2
- Reid, G., Lynch, J. P., Fishbein, M. C., & Clark, N. M. (2020). Mucormycosis. Seminars in Respiratory and Critical Care Medicine, 41(01), 099–114. doi:10.1055/s-0039-3401992









0 Comments